Reverse Shoulder Replacement
Summary: Total shoulder replacement surgery is a proven way to relieve pain and stiffness in advanced shoulder arthritis or to treat a severe shoulder fracture.
For many people who have a current or prior rotator cuff injury, a traditional anatomic total shoulder replacement may not be optimal. For these patients, a reverse total shoulder replacement is often the best option.

In this article:
- What is a reverse total shoulder replacement?
- How does it differ from a conventional replacement?
- What type of implant is used?
- Who is a good candidate?
- Who is not a good candidate?
- What type of doctor performs this surgery?
- How long does the surgery take?
- Will I need physical therapy after?
- How soon can I drive after surgery?
- How long does it take to recover?
- What are the limitations after surgery?
- What are the potential risks?
- How long does the implant last?
- What is the success rate?
- Why should I come to HSS?
- Key takeaways
What is a reverse total shoulder replacement?
A reverse total shoulder replacement, also known as reverse shoulder arthroplasty, is a surgical procedure used to treat severe shoulder problems. The surgery involves removing the damaged parts of the shoulder joint and replacing them with a specially designed artificial joint.
This surgery is different from a traditional anatomic shoulder replacement and is typically recommended for people who have certain shoulder conditions, such as massive rotator cuff tears. This new joint allows the shoulder to move more effectively, even if the rotator cuff muscles are not working properly.
What is the difference between reverse shoulder replacement and regular shoulder replacement?
The main difference is how the artificial joint is positioned in the shoulder. In a regular or traditional shoulder replacement (called an anatomic shoulder replacement), the damaged parts of the shoulder joint – the ball and socket – are replaced with artificial ones in the same positions as in the natural joint. In a reverse shoulder replacement, the positions of the ball and socket are switched. The artificial ball is attached to the socket side of the joint and the artificial socket is placed where the natural ball used to be.
By reversing the positions of the ball and socket, the surgery allows different muscles to take over the function of the damaged ones, improving the shoulder's movement and stability. This changes how the shoulder rotates at its center and utilizes different muscles, such as the deltoid, to provide better stability and movement, especially for individuals with compromised rotator cuff muscles or complex shoulder conditions.


Video: Reverse shoulder replacement animation
What type of implant is used for reverse shoulder replacement?
In a reverse shoulder replacement, the implant consists of two main components: The glenosphere and the humeral component.
- The glenosphere is the artificial ball component. It is made of metal – usually a metal alloy or titanium – and has a smooth surface to allow it to move freely. It replaces the damaged natural socket (glenoid) of the shoulder joint.
- The humeral component is the artificial socket. It is made of a durable plastic material called polyethylene. This component replaces the damaged natural ball – the humeral head (head of the humerus bone) – of the shoulder joint.
The materials used for the implant components are typically durable and biocompatible, meaning they are well-tolerated by the body and can withstand the stresses of everyday activities. Orthopedic surgeons choose the appropriate size and type of implant based on the patient's specific shoulder anatomy and the severity of their shoulder condition.
Who is a good candidate for reverse shoulder replacement?
A reverse shoulder replacement is usually recommended for people who have certain types of shoulder arthritis or more complex shoulder issues. Some common indications for a reverse shoulder replacement include:
- a massive rotator cuff tear.
- shoulder arthropathy (disease or degeneration of the joint).
- a failed previous replacement.
- a complex shoulder fracture.
Massive rotator cuff tears
If a person has a large and irreparable tear in the rotator cuff, it can lead to significant pain and loss of shoulder function. In such cases, a reverse shoulder replacement may be considered as it relies on different muscles (such as the deltoid) to move the arm, rather than the damaged rotator cuff muscles.
Rotator cuff arthropathy
This is a condition where there is both a massive rotator cuff tear and arthritis in the shoulder joint. Reverse shoulder replacement is often chosen for patients with this condition because it can address both problems and provide pain relief and improved function.
Failed previous shoulder replacement
If a previous shoulder replacement has been unsuccessful or has led to complications, a reverse shoulder replacement might be recommended as an alternative solution.
Complex fractures
In some cases of severe shoulder fractures that cannot be repaired using conventional methods, a reverse shoulder replacement may be considered.
It's essential for individuals considering this surgery to undergo a thorough evaluation by an orthopedic surgeon to determine if they are a suitable candidate for a reverse shoulder replacement. Factors like the individual's overall health, age, bone quality, and shoulder function will be taken into account to make an informed decision about the most appropriate treatment option. As with any surgery, there are risks and benefits, and the decision should be made collaboratively between the patient and their medical team.
Who is not a good candidate for reverse shoulder replacement?
While reverse shoulder replacement can be beneficial for many individuals with specific shoulder conditions, there are certain situations where it may not be the most suitable option. Individuals who have good rotator cuff function, an active infection, severe osteoporosis, poor general health, or unrealistic expectations for the outcome may not be good candidates for a reverse shoulder replacement.
Good rotator cuff function
If the rotator cuff muscles are functioning relatively well and can adequately move the arm, a reverse shoulder replacement may not be necessary. In such cases, a regular shoulder replacement can be considered, if the patient has painful arthritis and a functional rotator cuff. Or, other less invasive treatments may be more appropriate in patients who have not tried more conservative treatments.
Active infections
Active infections in the shoulder joint or surrounding tissues can increase the risk of complications after surgery. Infections need to be treated and resolved before considering any joint replacement procedure.
Severe osteoporosis
Severe osteoporosis or significant bone loss in the shoulder area may compromise the ability to anchor the artificial components securely. In such cases, the stability of the implant might be compromised. Severe osteoporosis can also substantially increase the risk of stress fractures in the shoulder blade after reverse shoulder replacement.
Poor general health
Individuals with other serious medical conditions that make surgery risky or difficult to recover from (such as severe heart or lung disease) may not be good candidates.
Unrealistic expectations
Patients who have unrealistic expectations about the outcome of the surgery or those who are not committed to participating in postsurgical rehabilitation and physical therapy may not be suitable candidates.
What type of doctor performs reverse shoulder replacement? How experienced should they be?
Reverse shoulder arthroplasty is performed by an orthopedic surgeon who specializes in shoulder reconstruction. This can include orthopedic surgeons with advanced training in shoulder and elbow surgery, sports medicine, hand and upper extremity surgery or orthopedic trauma surgery. The best outcomes after reverse shoulder arthroplasty are seen in orthopedic surgeons who perform a high volume of the procedure each year.
How long does the surgery take?
A reverse shoulder replacement can take between 1 to 3 hours to perform.
Will I need physical therapy? If so, for how long?
Both anatomic and reverse shoulder replacements require rehabilitation afterward to regain strength and mobility in the shoulder. Depending on a patient’s goals for activity, they may benefit from PT for 3 to 6 months after surgery.
When can I drive after reverse shoulder replacement?
Ask your doctor for their specific instructions but, on average, they may recommend:
- Waiting 2 to 4 weeks to allow for safe driving practices and reaction time, or
- Waiting until you are out of your sling, which can be 4 to 6 weeks
How long does it take to recover from reverse shoulder replacement?
The recovery time for a reverse shoulder replacement can vary depending on several factors, including the individual's age, overall health, the extent of the shoulder damage, and their commitment to post-operative rehabilitation. Both anatomic and reverse shoulder replacements require rehabilitation afterward to regain strength and mobility in the shoulder.
Generally, the recovery process can be broken down into several phases:
- Hospital stay: After reverse shoulder replacement, patients typically stay in the hospital overnight for one night for close monitoring and initial recovery.
- Early recovery (1 to 6 weeks): During the first few weeks after surgery, patients focus on pain management, wound healing, and gradually regaining shoulder movement. Physical therapy sessions are started to improve range of motion and strengthen the surrounding muscles.
- Mid recovery (6 weeks to 3 months): At this stage, patients continue with physical therapy to enhance shoulder strength, stability, and mobility. They may start using the arm for everyday activities with some restrictions and gradually increase their activity level.
- Late recovery (3 to 6 months): Around three months post-surgery, many patients experience significant improvement in shoulder function. Physical therapy, which can include home exercises, typically intensifies, focusing on building muscle strength and coordination for more complex movements and functional activities.
- Full recovery (6 to 12 months): By six months to a year after the surgery, most patients have achieved a significant recovery and can perform daily tasks with improved shoulder function. However, full recovery can continue beyond the one-year mark, with ongoing improvements in strength and range of motion.
It's important to note that individual recovery times can vary, and some people may take longer to reach their maximum potential. In order to maximize recovery potential, patients should adhere to the recommended rehabilitation program and follow the advice of the medical team. During the recovery period, patients should avoid heavy lifting, high-impact activities, and movements that put excessive strain on the shoulder joint. Following the surgeon's and physical therapist's instructions is essential to ensure a successful outcome and minimize the risk of complications.
What are the limitations after reverse shoulder replacement?
After a reverse shoulder replacement, patients may experience certain limitations, especially during the initial stages of recovery. These limitations can vary depending on individual factors such as the patient's age, overall health, the specific shoulder condition being treated, and the success of the surgery. Some common limitations include:
- Limited range of motion: While a reverse shoulder replacement can improve shoulder function, some patients may still experience limitations in their range of motion, particularly in certain directions. It may take time and consistent physical therapy to regain full shoulder mobility and, sometimes, complete restoration of range of motion may not be achieved. Also, after a reverse shoulder replacement, the scapula (shoulder blade) moves more to make up for reduced motion in the shoulder joint. It is not known how or if this change affects shoulder strength, comfort, or long-term function.
- Weight restrictions: Patients are often advised to avoid heavy lifting or activities that put excessive strain on the shoulder joint, especially during the early stages of recovery. Following the surgeon's weight restrictions is essential to prevent potential complications or implant damage.
- Strength and endurance: It can take several months to regain full shoulder strength and endurance after the surgery. Physical therapy and exercises are essential to help build and strengthen the surrounding muscles gradually.
It's important for patients to have realistic expectations about the limitations and recovery process after reverse shoulder replacement. Working closely with the orthopedic and physical therapy team, adhering to postoperative instructions, and maintaining a healthy lifestyle can help optimize the outcomes and minimize potential limitations. Each patient's experience is unique, and regular follow-up appointments with their orthopedic surgeon can address any concerns and ensure that the recovery is progressing as expected.
What are the potential risks of reverse shoulder replacement?
Reverse shoulder replacement, like any surgical procedure, carries certain risks and potential complications. Some of the potential risks associated with a reverse shoulder replacement include:
- infections
- implant loosening or dislocation
- shoulder fracture
- persistent pain
- limited range of motion
- allergic reaction to a prosthesis
- nerve or blood vessel damage
- anesthesia-related complications
Infection
There is a risk of infection at the surgical site, which can lead to pain, swelling, and, in severe cases, may require additional treatment or even revision surgery.
Implant loosening or dislocation
The artificial components used in the reverse shoulder replacement can potentially loosen or dislocate over time. This may cause instability and affect the functioning of the shoulder joint. This often may require revision surgery to address this.
Fracture
Fractures can occur around the implant site or around the shoulder blade during or after the surgery, especially in individuals with weaker bones or compromised bone structure. The most common postsurgical fractures occur in the acromion (bony point at the top of the shoulder) and scapular spine (a bony ridge on the back of the shoulder blade).
Persistent pain
Some patients may experience persistent pain or discomfort following the surgery, which may require further evaluation and management.
Limited range of motion
While reverse shoulder replacement can improve shoulder function, some patients may still have limitations in their range of motion, particularly in certain directions like behind the back.
Allergic reaction
In rare cases, patients may experience an allergic reaction to the materials used in the implant.
Nerve or blood vessel injury
During the surgery, there is a slight risk of damaging nearby nerves or blood vessels, which can lead to weakness, numbness, or circulation problems in the arm. Surgery also increases the risk of developing blood clots, which can be dangerous if they travel to other parts of the body, causing blockages. This risk is higher in people who have a prior history of blood clots or a family history of blood clots.
Complications with anesthesia
General anesthesia carries its own set of risks, including adverse reactions and breathing difficulties.
It's important to note that while these risks exist, many people undergo reverse shoulder replacement successfully with positive outcomes and without complications. The decision to proceed with the surgery should be made after thorough discussions with the patient’s orthopedic surgeon, who will carefully assess the patient’s overall health and specific shoulder condition and weigh the potential risks against the benefits of the procedure.
How long does a reverse shoulder replacement implant last?
According to some studies, the long-term survival rate of reverse shoulder replacements is around 85% to 90% at 10 years after the surgery.3, 18, 19 “Survival rate” means that the implant is still functioning well in the majority of patients at that time point. Newer advancements in implant design and surgical techniques continue to improve outcomes and longevity.
What is the success rate of reverse shoulder replacement?
The success rate of reverse shoulder replacement is generally high, with many patients experiencing significant improvement in pain relief and shoulder function. The procedure has been particularly successful in treating certain shoulder conditions, such as massive rotator cuff tears and rotator cuff arthropathy, where traditional shoulder replacements may not provide satisfactory results.
The success rate can vary depending on factors such as the patient's age, overall health and the specific shoulder condition being treated. However, research and clinical studies have shown favorable outcomes for many patients who undergo reverse shoulder replacement. Patient satisfaction rates after reverse shoulder placement have been reported as high as 90% to 95% at 10 years after their shoulder replacement.17
Why should I come to HSS for reverse shoulder replacement surgery?
As noted above, the best outcomes are shown to be achieved by surgeons who perform a high volume of this procedure each year. HSS surgeons perform more total shoulder replacements than are done at any other hospital in New York State – historically more than twice the number surgeries as the next highest-volume hospital.13 In a survey of people who had total shoulder replacement at HSS, 100% reported improvement within 12 months after their treatment.10 In addition, HSS has low complication rates for this surgery. One independent study demonstrated that the complication rate at HSS was more than 30% lower than the national average.6
Key takeaways
- Reverse shoulder replacement is designed for people who have severe shoulder arthritis or irreparable rotator cuff damage. Unlike standard shoulder replacement, it reverses the ball-and-socket positions so the deltoid muscle (instead of the rotator cuff) powers shoulder movement.
- It is most often recommended for people who have rotator cuff arthropathy (a rotator cuff tear plus shoulder arthritis), severe shoulder arthritis that is not amenable to anatomic shoulder replacement, failed prior replacements, or severe shoulder fractures.
- Recovery is gradual and requires rehabilitation. Patients usually need physical therapy for 3 to 6 months, with major recovery milestones between 3 to 12 months.
- Risks include infection, implant loosening, stress fracture, persistent pain, and limited range of motion, but most patients have good outcomes.
- Success rates are high, especially at high-volume orthopedic surgical centers, with patient satisfaction reported as high as 90% to 95% ten years after their surgeries.
Dr. Gabriella Ode is a board certified orthopedic surgeon specializing in sports medicine and shoulder surgery in the HSS Sports Medicine Institute with offices in Manhattan and Brooklyn. Her clinical practice specializes in shoulder and knee injuries. Dr. Ode has a particular interest in women's sports medicine and is a team orthopedic surgeon for the New York Liberty professional women's basketball team.
![]()
Authors

Explore Related Patient Stories
View All Patient Stories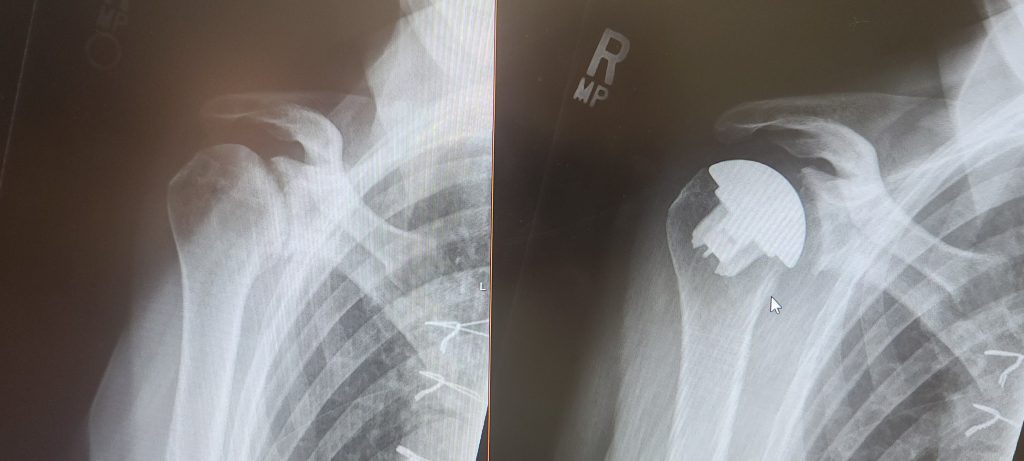
Dorothy Fortuna
Ridge, NY
Reverse Shoulder Replacement
Debbie Winchester
Rhinebeck, NY
Reverse Shoulder Replacement

Patricia Brawer
New York, NY
Reverse Shoulder Replacement

Jessica Bernstein
New Paltz, NY
Reverse Shoulder Replacement

Nancy Papa
Chester, NJ
Reverse Shoulder Replacement
Patrick Moletteri
Far Hills, NJ
Reverse Shoulder Replacement

David Curren
Boonton, NJ
Reverse Shoulder Replacement

Annalise Ferrara
Weston, CT
Reverse Shoulder Replacement

Arleene Ferko
Stamford, CT
Reverse Shoulder Replacement
Richard Poole
Richmond Hill, NY
Reverse Shoulder Replacement

Richard Albani
Jackson, NJ
Reverse Shoulder Replacement

Mary Beth Interlandi
Boca Raton, FL
Reverse Shoulder Replacement
References
- Beauperthuy AG, Linton NF, Falgiano PA, Mekkawy KL, Rodriguez HC, Gupta A. Reverse Shoulder Arthroplasty in Patients with Rheumatoid Arthritis: A Nationwide Analysis. J Clin Med. 2025 Feb 4;14(3):994. doi: 10.3390/jcm14030994. PMID: 39941664; PMCID: PMC11818557. https://pubmed.ncbi.nlm.nih.gov/39941664/
- Brusalis CM, Taylor SA. Periprosthetic Fractures in Reverse Total Shoulder Arthroplasty: Current Concepts and Advances in Management. Curr Rev Musculoskelet Med. 2020 Aug;13(4):509-519. doi: 10.1007/s12178-020-09654-8. PMID: 32506260; PMCID: PMC7340687. https://pubmed.ncbi.nlm.nih.gov/32506260/
- Chelli M, Boileau P, Domos P, Clavert P, Berhouet J, Collin P, Walch G, Favard L. Survivorship of Reverse Shoulder Arthroplasty According to Indication, Age and Gender. J Clin Med. 2022 May 10;11(10):2677. doi: 10.3390/jcm11102677. PMID: 35628804; PMCID: PMC9145012. https://pubmed.ncbi.nlm.nih.gov/35628804/
- Colasanti CA, Lin CC, Levin JM, Shen MS, Ben-Ari E, Alaia E, Simovitch RW, Zuckerman JD. Zone-specific bone density evaluation of the acromion may predict postoperative acromion stress fracture in patients undergoing a reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2025 Mar 13:S1058-2746(25)00214-9. doi: 10.1016/j.jse.2025.02.013. Epub ahead of print. PMID: 40089016. https://pubmed.ncbi.nlm.nih.gov/40089016/
- Davie RA, Nathan K, Persaud SG, Oladeji LO, Taylor SA, Dines JS, Fu MC, Ode GE, Dines DM, Gulotta LV, Brusalis CM. Inconsistent reporting of risk factors for acromial stress fractures following reverse total shoulder arthroplasty: a systematic review. J Shoulder Elbow Surg. 2025 Mar 28:S1058-2746(25)00254-X. doi: 10.1016/j.jse.2025.02.032. Epub ahead of print. PMID: 40158877. https://pubmed.ncbi.nlm.nih.gov/40158877/
- FAIR Health claims data (analysis of), January 2023 – June 2024 [cited 2025 Aug 24]. Complication rates: HSS rate 2.56% vs. national rate of 3.66%, during the period from January 1, 2023, through June 30, 2024. FAIR Health is a nonprofit organization whose mission is to supply reliable information for all stakeholders to improve health care quality, access and affordability. FAIR Health is not responsible for the conduct of the research or for any of the opinions expressed in this article.
See: https://www.fairhealthconsumer.org/quality and https://www.fairhealth.org/who-we-serve/research. - Franceschetti E, Giovannetti de Sanctis E, Gregori P, Palumbo A, Paciotti M, Di Giacomo G, Franceschi F. Return to sport after reverse total shoulder arthroplasty is highly frequent: a systematic review. J ISAKOS. 2021 Nov;6(6):363-366. doi: 10.1136/jisakos-2020-000581. Epub 2021 Mar 11. PMID: 34794965. https://pubmed.ncbi.nlm.nih.gov/34794965/
- Girdler SJ, Maza N, Lieber AM, Vervaecke A, Kodali H, Zubizarreta N, Poeran J, Cagle PJ, Galatz LM. Impact of Surgeon Case Volume on Outcomes After Reverse Total Shoulder Arthroplasty. J Am Acad Orthop Surg. 2023 Dec 15;31(24):1228-1235. doi: 10.5435/JAAOS-D-23-00181. Epub 2023 Oct 12. PMID: 37831947. https://pubmed.ncbi.nlm.nih.gov/37831947/
- Harkin W, Berreta RS, Williams T, Turkmani A, Scanaliato JP, McCormick JR, Klifto CS, Nicholson GP, Garrigues GE. The effect of surgeon volume on complications after total shoulder arthroplasty: a nationwide assessment. J Shoulder Elbow Surg. 2025 Apr;34(4):1112-1119. doi: 10.1016/j.jse.2024.07.025. Epub 2024 Sep 6. PMID: 39244148. https://pubmed.ncbi.nlm.nih.gov/39244148/
- Hospital for Special Surgery. HSS Internal Data, 2022. 100% of respondents to surveys known as patient-reported outcome measures (PROMS) reported improvement within 12 months. The number of survey respondents was 34, which represented a 74% response rate.
- Johnson MA, Cogsil T, White AE, Omurzakov A, Kontaxis A, Taylor SA, Dines JS, Fu MC, Ode GE, Ode GE, Gulotta LVDines DM, Gulotta LV, Brusalis CM. Impact of Reverse Total Shoulder Arthroplasty on Scapulohumeral Rhythm: A Systematic Review and Meta-Analysis. J Shoulder Elbow Surg. 2025 Sep 19:S1058-2746(25)00657-3. doi: 10.1016/j.jse.2025.08.010. Epub ahead of print. PMID: 40976550. https://pubmed.ncbi.nlm.nih.gov/40976550/
- Moverman MA, Puzzitiello RN, Glass EA, Swanson DP, Efremov K, Lohre R, Bowler AR, Mahendraraj KA, Le K, Dunn WR, Cannon DJ, Friedman LGM, Gaudette JA, Green J, Grobaty L, Gutman M, Kakalecik J, Kloby MA, Konrade EN, Knack MC, Loveland A, Mathew JI, Myhre L, Nyfeler J, Parsell DE, Pazik M, Polisetty TS, Ponnuru P, Smith KM, Sprengel KA, Thakar O, Turnbull L, Vaughan A, Wheelwright JC, Abboud J, Armstrong A, Austin L, Brolin T, Entezari V, Garrigues GE, Grawe B, Gulotta LV, Hobgood R, Horneff JG, Hsu JE, Iannotti J, Khazzam M, King JJ, Kirsch JM, Levy JC, Murthi A, Namdari S, Nicholson GP, Otto RJ, Ricchetti ET, Tashjian R, Throckmorton T, Wright T, Jawa A; ASES Complications of RSA Multicenter Research Group. Implant-Positioning and Patient Factors Associated with Acromial and Scapular Spine Fractures After Reverse Shoulder Arthroplasty: A Study by the ASES Complications of RSA Multicenter Research Group. J Bone Joint Surg Am. 2024 Aug 7;106(15):1384-1394. doi: 10.2106/JBJS.23.01203. Epub 2024 Jun 5. PMID: 40305832. https://pubmed.ncbi.nlm.nih.gov/40305832/
- New York State Department of Health. Hospital Inpatient Discharges (SPARCS De-Identified): 2017 [Internet]. Albany (NY): New York State Department of Health; [cited 2025 Aug 24]. Available from: https://health.data.ny.gov/dataset/Hospital-Inpatient-Discharges-SPARCS-De-Identified/22g3-z7e7. Surgical volume: HSS performed 369 total shoulder replacements in 2017, which was 247% more than the next leading hospital.
- North D, Hones KM, Jenkins P, Sipavicius E, Zermeño Salinas JL, Hao KA, Schoch BS, Wright TW, Gulotta LV, King JJ. How common is nerve injury after reverse shoulder arthroplasty? A systematic review. J Shoulder Elbow Surg. 2023 Apr;32(4):872-884. doi: 10.1016/j.jse.2022.10.022. Epub 2022 Nov 24. PMID: 36427756. https://pubmed.ncbi.nlm.nih.gov/36427756/
- Rauck RC, Swarup I, Chang B, Ruzbarsky JJ, Gulotta LVDines DM, Gulotta LVDines DMWarren RF, Henn RF 3rd, Gulotta LV. Preoperative patient expectations of elective reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2019 Jul;28(7):1217-1222. doi: 10.1016/j.jse.2018.12.008. Epub 2019 Mar 20. PMID: 30904239. https://pubmed.ncbi.nlm.nih.gov/30904239/
- Rossi LA, Tanoira I, Ranalletta M, Kunze KN, Farivar D, Perry A, Chahla J. Cemented vs. uncemented reverse shoulder arthroplasty for proximal humeral fractures: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2022 Mar;31(3):e101-e119. doi: 10.1016/j.jse.2021.10.011. Epub 2021 Nov 2. PMID: 34737086. https://pubmed.ncbi.nlm.nih.gov/34737086/
- Sheth MM, Heldt BL, Spell JH, Vidal EA, Laughlin MS, Morris BJ, Elkousy HA, Edwards TB. Patient satisfaction and clinical outcomes of reverse shoulder arthroplasty: a minimum of 10 years' follow-up. J Shoulder Elbow Surg. 2022 Apr;31(4):875-883. doi: 10.1016/j.jse.2021.09.012. Epub 2021 Oct 14. PMID: 34656776. https://pubmed.ncbi.nlm.nih.gov/34656776/
- Varvitsiotis D, Kokkineli S, Feroussis C, Apostolopoulos N, Zakilas D, Feroussis J. Long-Term Results of Primary Reverse Shoulder Arthroplasty for Massive, Irreparable Rotator Cuff Tears Without Glenohumeral Arthritis with a Mean Follow up of 9.4 Years. J Shoulder Elb Arthroplast. 2023 Aug 9;7:24715492231192072. doi: 10.1177/24715492231192072. PMID: 37575314; PMCID: PMC10413892. https://pubmed.ncbi.nlm.nih.gov/37575314/
- Watanabe S, Kaibara T, Feeley BT, Zhang AL, Lansdown DA, Ma CB. Survival rate and outcomes of reverse total shoulder arthroplasty with a minimum ten-year follow-up using a trabecular metal implant. Bone Jt Open. 2025 Oct 2;6(10):1171-1178. doi: 10.1302/2633-1462.610.BJO-2025-0147.R1. PMID: 41033667. https://pubmed.ncbi.nlm.nih.gov/41033667/