Hip Arthroscopy
Summary: Hip arthroscopy is a minimally invasive procedure in which orthopedic surgeons use flexible, fiber-optic tube with a small camera and surgical instruments to diagnose and/or treat a range of hip joint conditions. This article explains how hip arthroscopy works, its advantages over open surgery, and which hip conditions it can address. It explains recovery timelines and expectations, including physical therapy, and returning to pain-free activity.
On this page:
What is hip arthroscopy?
Hip arthroscopy, sometimes called a “hip scope,” is a minimally invasive procedure in which an orthopedic surgeon uses an arthroscope to examine the inside of the hip joint.
This procedure allows the surgeon to diagnose the cause of hip pain or other problems in your joint. Some hip conditions may also be treated arthroscopically. To perform arthroscopic hip surgery in these cases, the surgeon makes additional small incisions (usually one or two) to create access points for various arthroscopic needles, scalpels or other special surgical tools.
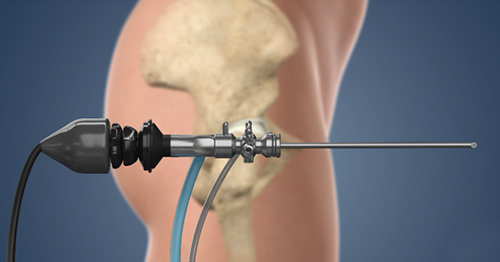
Hip arthroscopy video
View this step-by-step animation of a hip arthroscopy procedure.
What are the advantages of hip arthroscopy?
A hip scope has several advantages over traditional open hip surgery, because it:
- causes very little trauma to the joint (which minimizes hip pain and scarring)
- is generally done on an outpatient basis (where patients return home after the procedure)
- typically has a short recovery period
- may postpone the advancement of hip arthritis by treating its cause in the early stages
- can delay or eliminate the need for a hip replacement by preemptively treating conditions that cause osteoarthritis of the hip
Which hip conditions can be treated arthroscopically?
Common injuries and conditions that can be fixed with arthroscopic hip surgery are:
- hip impingement (femoroacetabular impingement), which limits range of motion and is a major cause of osteoarthritis
- repair or trimming of a labral tear, where a specialized cartilage called the labrum, which lines the hip socket becomes torn
- removal of:
- loose fragments of cartilage inside the joint (which are usually caused by an injury, such as a torn labrum)
- diseased or inflamed joint lining
- painful bone spurs
Is hip arthroscopy right for you?
Because HSS uses high-resolution MRI scanning technology, a hip arthroscopy is not always required to make a diagnosis. Our state-of-the-art scans may reveal that your injury or condition can be treated nonsurgically, such as with physical therapy. For this reason, at HSS, arthroscopic surgery is often performed only when reparative surgery is needed, rather than for exploratory purposes.
To determine whether a hip arthroscopy is right for your situation, your physician will first:
- learn about your symptoms and medical history
- review your imaging (X-rays, CT scans and/or MRIs)
- conduct a physical examination that may include range-of-motion tests
Overview of a hip arthroscopy procedure
Arthroscopic hip surgery is usually conducted on an outpatient basis, where the patient returns home on the same day as the surgery. Depending on your doctor's findings and the type of treatment that will be performed, arthroscopic hip surgery may take between 30 minutes and two hours.
Preparation
Prior to the procedure, you will be given anesthesia to prevent the sensation of pain. You may undergo general anesthesia, in which a gas puts you to sleep, or regional anesthesia, in which an injection or small tube (catheter) delivers medication to the spinal column, numbing you from the waist down. At HSS, more than 90% of hip arthroscopy procedures are performed under regional anesthesia, rather than general anesthesia. This lowers risks and decreases the time between surgery and a patient’s discharge from the hospital.
Most often, you will be positioned with your leg pulled in traction. This creates space in the hip joint and allows instruments to access the joint without injuring surrounding cartilage. Accessing the narrow space in the hip joint is complicated by the orientation of surrounding nerves and blood vessels. To ensure the arthroscope and instruments are inserted properly, a portable X-ray device called a fluoroscope will be positioned for use during the procedure.
Incisions and accessing the joint
Your surgeon will make two or three small, one-quarter to one-half inch long incisions called portals along pre-marked sites.
First, a needle will be inserted into the joint space, and when positioning is confirmed with the fluoroscope, the joint is injected with a sterile, water-based solution, creating fluid pressure to help hold open the joint. An incision is made, and a guide wire is passed through the needle, which is withdrawn.
Next, a thin tube, called a cannula, is inserted over the guide wire into the joint space. The wire is withdrawn, and an arthroscope is inserted through the cannula to visualize the joint. The other one or two portals are accessed similarly, and once complete, the location of the arthroscope or instruments can be changed to view the joint or repair tissues from a variety of positions. Fluid may be directed into and out of the joint through attachments on the arthroscope or via other portals to aid viewing inside the joint.
Diagnosis and surgical repairs
Typically, your surgeon will examine the condition of the articular cartilage that covers both the head of the hip ball (the femoral head, located at the top of your thighbone) and the inside the socket (the acetabulum). This cartilage allows the bone surfaces to slide against each other smoothly. Your surgeon will also examine the:
- condition of ligaments attaching the bones to each other
- the firm ring of cartilage surrounding the hip socket, called the labrum, to look for a hip labral tear
- space within the joint to determine whether there are loose bodies of cartilage material or signs of inflammation or degenerative conditions such as osteoarthritis
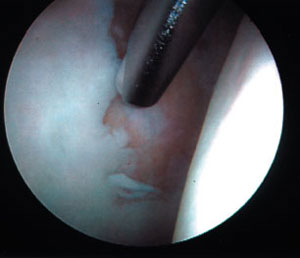
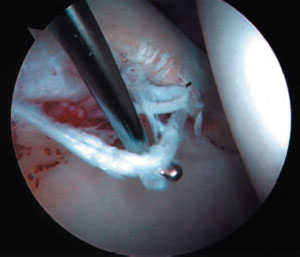
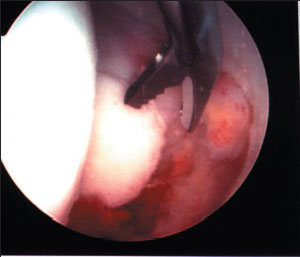
Fluoroscopic and arthroscopic images of hip arthroscopy

End of the procedure
Once exploration and any treatments are complete, your surgeon will withdraw the arthroscope and any other instruments. Your incisions may be closed with two to three non-dissolvable sutures and covered with small bandages, or they may be held closed with wound closure surgical tape strips.
You may be given a prescription for pain and directed to ice the area. Your doctor may also advise you on what to wear after hip arthroscopy, such as a brace and types of clothing to accommodate a brace. You may also need to walk on crutches or otherwise limit weightbearing on your leg for a period of time.
Hip arthroscopy recovery: How long does pain last after hip arthroscopy?
Symptoms often improve immediately following the procedure, but recurrence of some pain can occur as the irritated joint lining heals, and temporary tenderness in the hip and knee from the traction may occur.
You may also feel a sensation of water in the hip or hear gurgling noises resulting from the fluid used during surgery, but this will quickly be absorbed by the body. Swelling should subside within about a week and any sutures will typically be removed in seven to ten days. Your full recovery time may vary, depending on the specific treatment performed during your procedure.
Hip arthroscopy patients must usually use crutches for one or two weeks after surgery and do six weeks of physical therapy. It may be three to six months before they experience no pain after physical activity.
Key takeaways
- Hip arthroscopy is a minimally invasive procedure used to diagnose and treat hip joint problems.
- The surgery typically involves small incisions, specialized instruments, and an arthroscope (camera) to view and repair tissues.
- Common conditions treated include hip impingement, labral tears, loose cartilage, and bone spurs.
- Most patients go home the same day and begin physical therapy within a few weeks.
- Full recovery and return to pain-free activity can take 3 to 6 months, depending on the treatment performed.
In the news
- Living Life to the Fullest: Multiple Joint Replacements Enable 73-year-old “Bionic Man” to Maintain Athletic Lifestyle
- 5 joint replacement surgeons to watch
- Meet 5 leaders in outpatient joint replacement surgery
- Top New York surgeon: Americans have better data for choosing restaurants than surgeons. That has to change
- Patients with iodine-related allergies may still receive iodine-based products during TJA
- COX-2 inhibitors, anticoagulants may not increase wound-related bleeding after THA.
- Computer navigation, robotic assistance may not increase PJI risk in TJA
- Direct anterior vs. posterolateral robotic-assisted THA
- Dual mobility THA yields similar dislocation, revision risks vs. metal, ceramic heads
- Computer-assisted fluoroscopy-based navigation reduced readmissions after THA
- Novel Nerve Block Combination Decreases Opioid Use, Enables Earlier PACU Discharge Times After Hip Arthroscopy
- Peripheral Nerve Blocks in Total Joint Arthroplasty May Provide the Best Reduction in Complications in Older Patients With Fewer Comorbidities
- Garrett Whitlock undergoes successful surgery
- Boston Bruins Issue Update On Brad Marchand
- Combination of Two Novel Nerve Blocks Reduces Opioid Use After Hip Arthroscopy
- HSS presents new research at 2022 ASRA Annual Meeting
- ACR Updates Guideline for Medication Management in Hip or Knee Arthroplasty
- HSS STUDY: “COMPREHENSIVE” GUIDE TO ACETABULAR COMPONENTS, LINERS
- New HSS Study Finds Hip Replacements on the Rise Among Adolescents Under 21 Years of Age
- Augmented reality puts holograms, data at fingertips of surgeons
- Hip Resurfacing vs. Total Arthroplasty: New Data
- MRI tracks soft-tissue complications after hip replacement
- High revision, conversion rates found among young and old patients after hip arthroscopy
- Bruins Issue Update On John Moore
- Castellano to have arthroscopic leg surgery; will return at Gulfstream
- Dissatisfied Hip Arthroscopy Patients? Might be Lumbosacral Transitional Vertebrae
- Stars provide updates on offseason surgeries for Bishop, Seguin
- Bruins Issue Update On Offseason Surgeries
- Hip arthroscopy for OA associated with high THA conversion rate
- Hip Arthroscopy for Arthritis Associated with Unacceptably High Conversion to Total Hip Replacement and Significantly Worse Outcomes
- Saving Careers, One Hip at a Time