Discectomy
Medically reviewed by Sohrab Virk, MD, MBA
A discectomy (also sometimes spelled diskectomy) is a form of spinal decompression surgery used to alleviate pain caused by a herniated disc, which occurs when a portion of a spinal disc bulges or ruptures and slips out of place. This can put pressure on a spinal nerve and, in turn, cause neck pain, back and/or leg pain (as may be felt in sciatica), leg weakness, leg numbness or cauda equina syndrome.

What is a discectomy vs. a laminectomy?
Both are spinal decompression surgeries that remove pressure on a nerve. The difference is what body is being removed. A discectomy incises and removes protruding soft vertebral disc tissue and only a portion of the bony lamina in the back of the spine. A laminectomy involves removing the majority of the lamina and may or may not involve removing a protruding disc.
How is a discectomy performed?
There are several variations of technique and surgical approaches. Regardless of the technique used by the surgeon, the vital portion of the procedure is removing the protruding disc that is placing pressure on nerves in the spine. The discussions below focus on lumbar discectomy techniques and approaches.
Discectomy techniques
Open discectomy
Although more minimally invasive techniques have emerged in recent decades, open discectomy surgery remains common. It involves a 3cm to 4cm incision per level of surgery (the number of vertebrae involved).
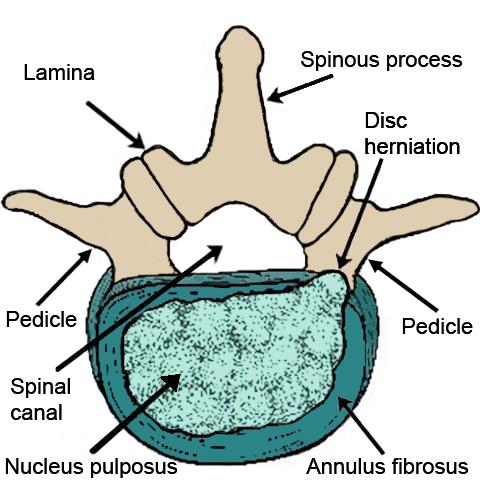
Overhead illustration of a lumbar vertebra with a herniated disc
It can be used for cases where there are there are herniations of several discs in multiple levels of the spine or when a patient also has complicated spine anatomy due to scoliosis or kyphosis. In an open surgery, an incision is made in the skin and muscle, and other soft tissues are moved aside to expose the spine.
Microdiscectomy
Microdiscectomy is less invasive than open spine surgery, as it involves a smaller incision and the use of a microscope or surgical magnifying glasses to visualize the site.
Endoscopic discectomy
Broadly, this refers simply to any discectomy in which the surgeon uses an endoscope (a narrow tube with a camera and light at the end) to directly view the herniated disc and surrounding structures during surgery. This procedure allows for the smallest possible incision for a discectomy (usually less than 1cm). It may involve an incision down the center of the back or an incision 10cm to 12cm from the center of the spine. A patient’s particular disc herniation dictates where the incision is made.
Surgical approaches for lumbar discectomy
There are two access angles through which a discectomy may be performed, depending on the patient’s case. These are the:
- Posterior approach (through the back of the spine).
- Transforaminal approach. This is at an angle (somewhat posterior and lateral) to access the disc through a spinal foramen. The foramen (plural, “foramina”) is the opening where nerves exit the spine. For example, a percutaneous transforaminal endoscopic discectomy is a minimally invasive discectomy through a small opening in the skin and into one or more foramina, using an endoscope for visualization.
How long does a discectomy take?
The procedure may take anywhere from as little as 45 minutes to about two hours, depending on the case and which discectomy technique and approach is used.
What complications can occur with discectomy?
All surgeries come with risks, although the most severe complications are rare. Possible complications can include blood clots, bleeding or infection at the surgical site, nerve injury, or a tear in the dural lining of the spinal cord resulting in a cerebrospinal fluid (CSF) leak. In rare cases, a vertebra immediately above or below that treated in the surgery may degenerate and lead to instability of the spine, and possibly additional surgery.
In addition, sometimes, a discectomy does not provide the intended relief of back pain or leg pain (from sciatica). This may lead to a desire for a second operation or to nonsurgical pain management treatments. Lastly, a treated disc can reherniate (reported in about 6% of cases), but the risk can be reduced by carefully following the postsurgical guidance.
To help avert a subsequent herniation of the treated disc, you should progressively resume light, then moderate activity on a schedule determined with your surgeon and physical therapist. Any return to heavy physical labor or contact sports must be made cautiously and only once approved by your healthcare team.
What is the discectomy recovery time?
Recovery times vary widely, depending on the severity of your condition, which type of discectomy procedure you have, as well as other factors such as your age, general health and lifestyle. For example, a discectomy performed in conjunction with a spinal fusion usually involves a longer recover periods than that of a discectomy alone.
One study at HSS found that more than 90% of patients returned to driving within two weeks after a microdiscectomy. There is also recent evidence that microdiscectomy patients can return to physical therapy and low impact aerobic exercise within four weeks after surgery.
In general, your discectomy may be done as an outpatient (same-day) procedure, or you may need to stay one or two nights in the hospital. You will resume walking as soon as possible and continue for about 2 to 4 weeks before resuming other activities, which will include physical therapy. Postsurgical pain should subside between 4 to 6 weeks. By about 8 to 12 weeks, most patients are able to return to all daily activities and, by three months, to more rigorous exercise and physical labor. A return to competitive sports activity, especially high impact sports such as football may take longer. Otherwise, most people will have made a full recovery by six months, with a minority taking as much as a year.
How successful is discectomy?
Widely varying success rates are reported by different institutions and studies, and the quality of what “success” means is subjective. However, a good measure of surgical success is measured is patients’ patients’ reported relief of pain after surgery and whether or not any additional surgery was required. Some research on discectomy patients at HSS that suggest success rates of more than 85%.
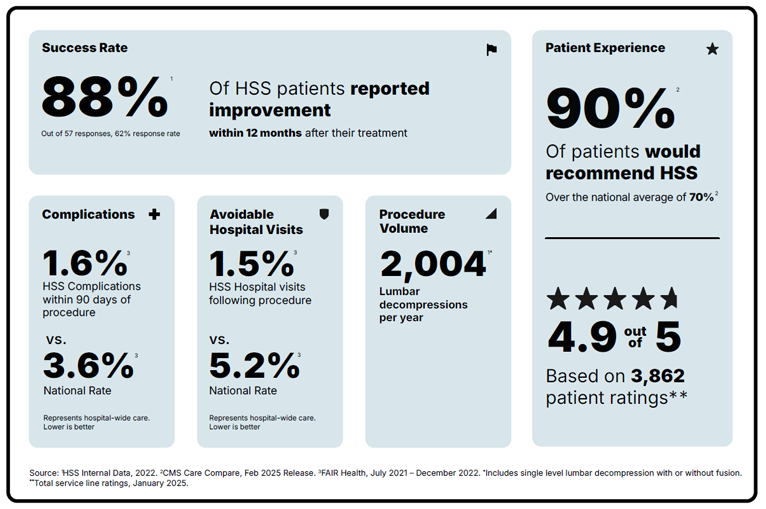
Lumbar discectomy for lower back pain has reported success rates of 60% to 90%. A study of more than 20,000 lumbar discectomy patients at HSS reported we had a success rate of about 88%, based on less than 12% of patients requiring any additional surgeries for their condition eight years after their discectomy.
Shared decision making for surgical success
In general, optimal outcomes require good, patient-centered care that rests on a foundation of shared decision-making between a doctor and a well-informed patient. Multiple degenerative and acute spinal disc conditions can reduce your quality of life and most require a multimodal therapeutic approach, with surgery being a last resort. The decision to have spine surgery is not easy.
Talk to your surgeon to make sure you understand your condition. Explain your expected outcomes for surgery – levels of pain reduction, improved function, a desire to return to a specific activity, concerns about subsequent surgeries, etc. – and find out whether discectomy or other surgical alternatives (such as a disc replacement) may best suit your case. Your surgeon has a responsibility to provide accurate and appropriate counseling to ensure you have all the information you need before opting for discectomy surgery.
Key takeaways
- A discectomy is a type of orthopedic surgeryperformed to remove a portion of a spinal disc that is placing pressure on a spinal nerve.
- There are a variety of techniques, including open surgery and minimally invasive tubular and endoscopic approaches. A spine surgeon will determine the ideal technique for a patient’s individual anatomy and injury.
- Recovery time: It usually takes 2 to 4 weeks to return to basic daily activities with continual progression to around three months for heavier exercise. Getting back to playing competitive sports may take longer.
Why choose HSS for lumbar spinal decompression surgery?
Lumbar spinal decompression is a surgery focused on reducing pain and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding these data points will help you make the best decision for your care: See hospital reliability data
Explore Related Patient Stories
View All Patient Stories
Donna Fennikoh
Brooklyn, NY
Degenerative Disc Disease
Marina Asher
Brooklyn, NY
Microdiscectomy: Minimally Invasive Surgery for a Herniated Disc
David G
New York, NY
Spine Surgery
Steven Lazerus
Commack, NY
Herniated Disc (Bulging Disc)
Marielaina Gless
Massapequa, NY
Nancy Guerriere
Hackettstown, NJ
Spine Surgery

Jon Lederer
Forest Hills, NY

Penny Love Hoff
Old Greenwich, CT
Hip Replacement

John Curran
Armonk, NY
Spine Surgery

Howard Waldrop
Mahwah, NJ
ACDF Surgery: Anterior Cervical Discectomy and Fusion

Karen Flynn
Massapequa Park, NY

Olga Bello-Lopez
Franklin Lakes, NJ
Spinal Fusion

Michael Quinn
Port Washington, NY
Rehabilitation

Theron Sweet
Syracuse, NY
ACDF Surgery: Anterior Cervical Discectomy and Fusion

Myles McGinley
New York, NY
Josephine Moore
New Windsor, NY
Spinal Stenosis
Dore Normile
New York, NY

Liliana Teran
Guadalajara, Mexico

Gavin Wolfe
New York, NY
Wendy Davis
Brooklyn, NY
Spinal Stenosis
References
- Altorfer FCS, Avrumova F, Abjornson C, Lebl DR. Cervical Disk Arthroplasty: Updated Considerations of an Evolving Technology. J Am Acad Orthop Surg. 2024 Jul 18. doi: 10.5435/JAAOS-D-24-00127. Epub ahead of print. PMID: 39029103. https://pubmed.ncbi.nlm.nih.gov/39029103/
- Dalal SS, Dupree DA, Samuel AM, Vaishnav AS, Gang CH, Qureshi SA, Bumpass DB, Overley SC. Reoperations after primary and revision lumbar discectomy: study of a national-level cohort with eight years follow-up. Spine J. 2022 Dec;22(12):1983-1989. doi: 10.1016/j.spinee.2022.06.005. Epub 2022 Jun 18. PMID: 35724809. https://pubmed.ncbi.nlm.nih.gov/35724809/
- Lebl DR, Meyers KN, Altorfer FCS, Jahandar H, Pazionis TJC, Nguyen J, O'Leary PF, Wright TM. Biomechanical Motion Changes in Adjacent and Noncontiguous Segments Following Single-Level Anterior Cervical Discectomy and Fusion: A Computed Tomography-Based 3D Motion Capture Study. Int J Spine Surg. 2024 Jul 4;18(3):249-257. doi: 10.14444/8605. PMID: 38866587. https://pubmed.ncbi.nlm.nih.gov/38866587/
- Phillips FM, Coric D, Sasso R, Lanman T, Lavelle W, Lauryssen C, Albert T, Cammisa F, Milam RA. Prospective, multicenter clinical trial comparing the M6-C compressible cervical disc with anterior cervical discectomy and fusion for the treatment of single-level degenerative cervical radiculopathy: 5-year results of an FDA investigational device exemption study. Spine J. 2024 Feb;24(2):219-230. doi: 10.1016/j.spinee.2023.10.020. Epub 2023 Nov 10. PMID: 37951477. https://pubmed.ncbi.nlm.nih.gov/37951477/
- Shahi P, Vaishnav AS, Mai E, Kim JH, Dalal S, Song J, Shinn DJ, Melissaridou D, Araghi K, Urakawa H, Sivaganesan A, Lafage V, Qureshi SA, Iyer S. Practical answers to frequently asked questions in minimally invasive lumbar spine surgery. Spine J. 2023 Jan;23(1):54-63. doi: 10.1016/j.spinee.2022.07.087. Epub 2022 Jul 15. PMID: 35843537. https://pubmed.ncbi.nlm.nih.gov/35843537/
- Subramanian T, Kaidi A, Shahi P, Asada T, Hirase T, Vaishnav A, Maayan O, Amen TB, Araghi K, Simon CZ, Mai E, Tuma OC, Eun Kim AY, Singh N, Korsun MK, Zhang J, Allen M, Kwas CT, Kim ET, Sheha ED, Dowdell JE, Qureshi SA, Iyer S. Practical Answers to Frequently Asked Questions in Anterior Cervical Spine Surgery for Degenerative Conditions. J Am Acad Orthop Surg. 2024 Apr 30. doi: 10.5435/JAAOS-D-23-01037. Epub ahead of print. PMID: 38709837. https://pubmed.ncbi.nlm.nih.gov/38709837/
- Virk SS, Diwan A, Phillips FM, Sandhu H, Khan SN. What is the Rate of Revision Discectomies After Primary Discectomy on a National Scale? Clin Orthop Relat Res. 2017 Nov;475(11):2752-2762. doi: 10.1007/s11999-017-5467-6. Epub 2017 Aug 28. PMID: 28849429; PMCID: PMC5638742. https://pubmed.ncbi.nlm.nih.gov/28849429/