Spinal Fusion Surgery
Medically reviewed by William D. Zelenty, MD
Summary: This page reviews spinal fusion surgery, an operation that can relieve pain, restore spinal stability, and correct deformities. Readers will learn which conditions it treats, get an overview of surgical techniques, and find links to articles on specific procedures. Also discussed are recovery timelines, risks, success rates, and the importance of individualized surgical care.

The number of spinal fusion procedures performed worldwide has increased dramatically in recent decades, due in large part to advancements in techniques, spinal implants, bone grafting materials, and innovations in surgical approaches. In addition, it has also become an appropriate surgical option to treat a broader number of spinal conditions.
On this page:
- What is spinal fusion surgery?
- What conditions require spinal fusion surgery?
- How does it work?
- How long is the hospital stay?
- Will I be able to drive again?
- How long after can I start to walk?
- How long is the recovery?
- Are there any permanent restrictions?
- What are the risks or complications?
- What is the success rate?
- Key takeaways
What is spinal fusion surgery?
Spinal fusion surgery is a procedure in which two or more vertebrae are fused together to either realign them or eliminate movement between them. It corrects a spinal deformity (improper curvature), relieve pain caused by vertebrae that are rubbing together, and restore stability when vertebrae have slipped out of place.
What requires a spinal fusion?
Spinal fusion surgery was originally developed for, and continues to be used as, a treatment for spinal instability, deformities (such as scoliosis and kyphosis), and traumatic spine fractures. However, it is now also used to treat a wider range of issues, such as degenerative disc disease, spondylolisthesis, and spinal tumors.
In many cases, non-operative treatments (such as physical therapy, epidural steroid injections or radiofrequency ablation) will be tried first. But if these measures fail to control back pain, neck pain, or potential neurological symptoms associated with degenerative processes in the spine, spinal fusion can be very effective in relieving symptoms by eliminating motion in the affected segment of the spine.
Conditions treated with spinal fusion surgery
- Degenerative disc disease (DDD) is where intervertebral spinal discs and/or facet joints deteriorate and lose function.
- Spinal fractures can result from either traumatic injury or from degenerative conditions such as osteoporosis or osteoarthritis. Fractures can lead to deformity or instability in the spine.
- Deformities of the spine include conditions like scoliosis and kyphosis. These deformities may be present at birth, develop during puberty, or result from injuries or certain genetic disorders in adults. They also may develop due to conditions like neuromuscular disease or osteoporosis.
- Spondylolisthesis is a type of mechanical instability of the spine. In this condition, the vertebrae slip forward and press on the spinal cord. It can cause pain not only in the lower back but also in the buttocks and legs. Spondylolisthesis is more common in people who have participated in high-impact sports like football, weightlifting, and gymnastics. It also tends to run in families. Spondylolisthesis can be caused by the degeneration of one or more facet joints or by a fracture of the pars interarticularis, a bony structure which connects the facet joints of the spine. (This is known as a pars fracture or spondylolysis.)
How does spinal fusion surgery work?
In spinal fusion surgery, surgeons place grafts (bone harvested from your own body, donor tissue or, sometimes, artificial bone ) that, over time cause the bone in two spinal vertebrae to grow into one another (fusion). Depending on which procedure is performed, they may use interbody devices (cages) that deliver bone materials and/or growth factors (artificially engineered versions of natural proteins that regulates bone healing) to the space between vertebra to generate fusion. Grafts can be placed in other locations as well, such as between the transverse processes of the vertebra or in the facet joints. Screws coupled to rods may be used to stabilize the vertebrae while new bone is growing.
Several minimally invasive techniques are available, for example endoscopic surgery. This technique involves visualization through an endoscope (a narrow tube) to access the spine to decompress and/or stabilize the spine. The advantage of this approach is to minimize muscle and soft tissue injury during surgery, usually also minimizing postoperative pain.
Before spinal fusion surgery, you may be screened with a test called a dual-energy x-ray absorptiometry (DEXA) or quantitative computed tomography scan (CT scan). This gives your doctors the ability to measure bone density within your vertebra. You may be given hormones and other medications for several months before or after your surgery to improve the strength of your bones and their ability to regrow.
How long is a hospital stay after spinal fusion?
Some patients – usually those having a minimally invasive spinal fusion – can return home on the same day as their surgery, but most will spend one or two nights in the hospital. Those with comorbidities (additional health problems, such as sleep apnea or a history of blood clots), who are having a complex fusion surgery or experience postsurgical complications may stay up to four or more nights.
Will I be able to drive again after spinal fusion surgery?
Most people who have spinal fusion surgery are able to return to driving, about three weeks or more after surgery. You should consult your surgeon for their specific protocols.
How long does it take to walk after spinal fusion surgery?
This varies from individual to individual, however, patients are encouraged to start walking as soon as possible. In some cases, this is on the same day of surgery under the care and guidance of a physical therapist. Depending on your condition and/or need for walking aids prior to surgery, you may require a walking aid such as cane or walker for the first several weeks after surgery.
How long is the recovery from spinal fusion surgery?
Spinal fusion surgery recovery times depend on the specific type of fusion procedure that is performed. In a study of patients who underwent either minimally invasive lumbar laminectomy (MI-L) or minimally invasive TLIF (MI-TLIF) surgeries, more than 90% of those in the first category and more than 85% of those in the second returned to work between two and four weeks. However, for some patients, full recovery can take up to six months. Your surgeon and physical therapist can advise on your particular case.
During the recovery period, you may be restricted from certain activities such as bending or twisting the low back and lifting more than 15 to 20 pounds at a time. Depending on your surgeon’s protocol, these restrictions may be gradually relaxed over the course of six weeks to several months. You will be encouraged to gradually increase your level of cardiovascular activity by walking, stationary cycling, or using an elliptical machine. When restrictions are lifted you can work on strengthening your core and doing other exercises to increase your range of motion.
Are there permanent restrictions after spinal fusion surgery?
After your recovery period is over and you have healed from spinal fusion surgery, there are no restrictions on your activities.
What are the risks or complications of spinal fusion?
All surgical procedures carry some level of risk. There are a few main categories of risk when discussing spine surgery, including risk associated with anesthesia or risk of: infection, blood loss, damage to important anatomic structures (such as nerves, blood vessels, joints), or of developing additional spinal issues in the future. Because each individual has their own inherent risk profile and each surgery carries unique risks, it is best to discuss these topics with your surgeon directly.
Reduced risks at HSS
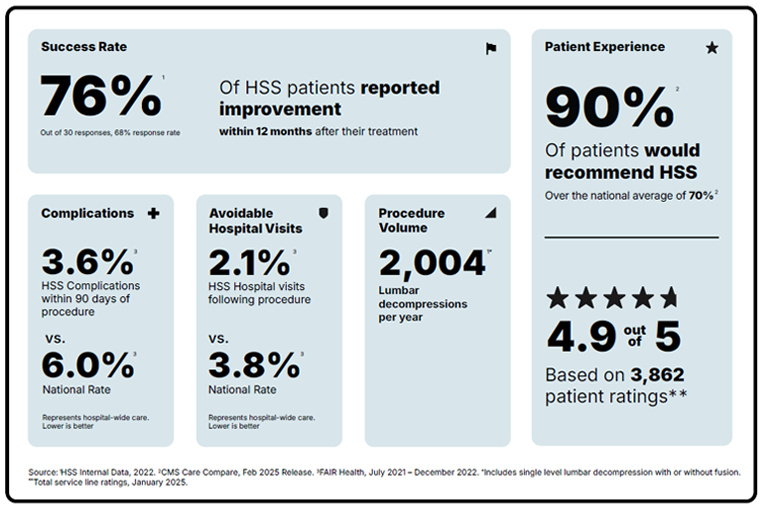
An independent, third-party study of lumbar decompression and fusion surgeries demonstrated that Hospital for Special Surgery had complication rates 40% lower than the national rate and postsurgical hospitalization rates of 45% lower than the national rate.2
What is the success rate of spinal fusion surgery?
Success after surgery can be measured in many ways. From a patient’s perspective, success might be relief of pain, improvement in neurologic function, and return to certain activities. Other measures of success include healing of the surgical wound, complete bony fusion, and degree of correction of a spinal deformity, among others. Because each scenario is unique it is best to discuss these topics with your surgeon directly.
Patients recommend HSS more
Data collected by the Centers for Medicare & Medicaid Services for lumbar spinal decompression and fusion surgery found that 89% patients recommended HSS, as compared to the national average of only 69%.1
Key takeaways
- Spinal fusion surgery stabilizes the spine by fusing vertebrae, eliminating motion, correcting deformities, and relieving pain. Conditions it can treat include:
- degenerative disc disease
- spinal fractures
- spinal deformities (scoliosis, kyphosis)
- spondylolisthesis
- certain spinal tumors
- Surgical technique: Grafts are used to promote bone fusion, while rods and screws may stabilize vertebrae during healing.
- Hospital stays usually range from 1 to 2 nights. Same-day discharge is possible for some people having a minimally invasive procedure. A complex case may require a stay of more than two nights.
- Early mobilization: Walking is encouraged soon after surgery and driving is generally possible after about three weeks, depending on the surgeon's guidance.
- Recovery timeline: Most patients return to work in 2 to 4 weeks for minimally invasive procedures, but full recovery can take up to six months.
- Risks and complications include infection, blood loss, nerve or vessel injury, anesthesia risks, and potential future spinal issues. Individualized risk assessment is essential.
- Success rates are measured by pain relief, improved neurological function, return to activities, bony fusion, or correction of spinal deformity.
Why choose HSS for lumbar decompression and fusion surgery?
Lumbar spinal decompression with fusion is a surgery focused on reducing pain and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding these data points will help you make the best decision for your care: See hospital reliability data
Learn more from the articles below.
References
- Centers for Medicare & Medicaid Services. Care Compare [Internet]. Baltimore (MD): CMS; 2023 Jul [cited 2023 Aug 9]. Available from: https://www.medicare.gov/care-compare/
- FAIR Health claims data (analysis of), July 2021 – December 2022 [cited 2023 Aug 9]. Data collected on lumbar decompression and fusion procedures demonstrated that HSS had a complication rate within 90 days of a procedure of 3.6% vs. national rate of 6.0%. HSS also had 2.1% rate of postsurgical hospital visits vs. a national rate of 3.8%. FAIR Health is a nonprofit organization whose mission is to supply reliable information for all stakeholders to improve health care quality, access and affordability. FAIR Health is not responsible for the conduct of the research or for any of the opinions expressed in this article. See: https://www.fairhealthconsumer.org/quality and https://www.fairhealth.org/who-we-serve/research.
- Khormaee S, Samuel AM, Schairer WW, Derman PB, McLawhorn AS, Fu MC, Albert TJ. Discharge to inpatient facilities after lumbar fusion surgery is associated with increased postoperative venous thromboembolism and readmissions. Spine J. 2019 Mar;19(3):430-436. doi: 29864544. 10.1016/j.spinee.2018.05.044. Epub 2018 Jun 2. PMID: 29864544.
https://pubmed.ncbi.nlm.nih.gov/29864544/ - Reisener MJ, Pumberger M, Shue J, Girardi FP, Hughes AP. Trends in lumbar spinal fusion-a literature review. J Spine Surg. 2020 Dec;6(4):752-761. doi: 10.21037/jss-20-492. PMID: 33447679; PMCID: PMC7797794. https://pubmed.ncbi.nlm.nih.gov/33447679/
- Shahi P, Vaishnav AS, Mai E, Kim HJ, Dalal S, Song J, Shinn DJ, Melissaridou D, Araghi K, Urakawa H, Sivaganesan A, Lafage V, Qureshi SA., Iyer S. Practical answers to frequently asked questions in minimally invasive lumbar spine surgery. Spine J. 2023 Jan;23(1):54-63. doi: 10.1016/j.spinee.2022.07.087. Epub 2022 Jul 15. PMID: 35843537.
https://pubmed.ncbi.nlm.nih.gov/35867600/ - Shinn D, Mok JK, Vaishnav AS, Louie PK, Sivaganesan A, Shahi P, Dalal S, Song J, Araghi K, Melissaridou D, Sheha ED, Sandhu HS, Dowdell JE 3rd, Iyer S, Qureshi SA.. Recovery Kinetics After Commonly Performed Minimally Invasive Spine Surgery Procedures. Spine (Phila Pa 1976). 2022 Nov 1;47(21):1489-1496. doi: 10.1097/BRS.0000000000004399. Epub 2022 Jul 15. PMID: 35867600.
https://pubmed.ncbi.nlm.nih.gov/35867600/ - Subramanian T, Araghi K, Sivaganesan A, Shahi P, Vaishnav A, Iyer S, Qureshi SA.. Ambulatory Lumbar Fusion: A Systematic Review of Perioperative Protocols, Patient Selection Criteria, and Outcomes. Spine (Phila Pa 1976). 2023 Feb 15;48(4):278-287. doi: 10.1097/BRS.0000000000004519. Epub 2022 Nov 4. PMID: 36692157. https://pubmed.ncbi.nlm.nih.gov/36692157/