Limb Lengthening Surgery
Medically reviewed by S. Robert Rozbruch, MD
A limb length discrepancy, in which one arm or leg is shorter than the other, can make it challenging to walk or perform everyday tasks. A significant leg length discrepancy can also lead to other medical problems with the knees, hips or spine, such as functional scoliosis. Limb lengthening is a major advance in orthopedic surgery over recent decades that can equalize limb lengths and enhance people's mobility.
What is a limb length discrepancy?
Limb length discrepancy (also called anisomelia) is a condition where one arm or leg is shorter than the other. It can affect both children and adults. The lower limbs are more commonly affected than the upper extremities, and this is called leg length discrepancy or short-leg syndrome.
- Having legs of unequal length creates an imbalance in posture and gait (the manner in which a person walks) that places stress on the low back and hip. This, in turn, causes pain and joint degeneration, which can include premature osteoarthritis.
- Having arms of different lengths creates asymmetry, which can lead to back and shoulder pain.
What is limb lengthening surgery?
Limb lengthening surgery is an orthopedic procedure to help people who have one arm or leg that is shorter than the other. It uses the body's own capacity to regenerate new bone as well as the soft tissues, ligaments, blood vessels, and nerves that surround and support it.
How does limb lengthening work?
Limb lengthening works by cutting a bone in half and then separating the two sections to allow new bone to grow into the space between them, a process known as "distraction osteogenesis." This revolutionary surgical concept reversed the long-held belief that bone could not be regenerated. In fact, bone has a natural ability to regenerate (grow more bone), for example, after either fracturing or being surgically cut (osteotomy). Limb lengthening surgery simply takes advantage of the osteogenesis mechanism.
In this way, bone segments can be lengthened by 15% to 100% of their original length. A bone is usually lengthened at a rate of about one millimeter (1 mm) per day. The lengthening phase of treatment (distraction) is followed by mineralization and hardening (consolidation) of the new bone. Soft tissues including skin, muscles, nerves, blood vessels stretch and grow during this process.
The complete process involves three steps – a surgery followed by two recovery phases:
- Surgery: An osteotomy (bone cut) is performed to divide the bone into two halves.
- Distraction phase: The two bone segments are slowly distracted (pulled apart) at a controlled rate and rhythm by way of either internal lengthening nails or external fixators.
- Consolidation and healing phase: New bone fills in the gradually enlarging gap that is created.
Distraction phase
During the distraction phase, the bone that has been cut into two is, very gradually, pulled apart in a process that promotes "distraction osteogenesis" – new bone growth at the site of the osteotomy. Continued growth of new bone tissue is accomplished by distracting, increasing the gap typically four times a day, one quarter millimeter (¼ mm) with each adjustment, for a total of one millimeter (1 mm) a day.
During this phase, additional strategies are available to correct any deformity that may be present, such as a misalignment of the bone resulting from trauma, a birth defect or other condition such as bowleg or knock knee . Early on in this phase, patients walk with the aid of crutches in order to remain mobile.
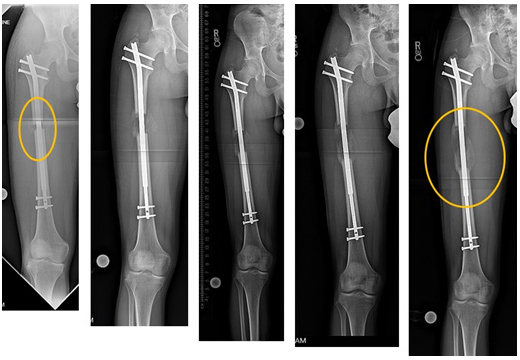 X-ray images of an osteotomy of the femur performed through a percutaneous approach over a three-month period. Gradual lengthening (8 cm) was accomplished with an internal lengthening nail to optimize leg lengths. Note the early new bone formation in the gap.
X-ray images of an osteotomy of the femur performed through a percutaneous approach over a three-month period. Gradual lengthening (8 cm) was accomplished with an internal lengthening nail to optimize leg lengths. Note the early new bone formation in the gap.As the space between the ends of the bone opens up, the body continues to produce new tissue in the gap until the desired length of bone has been generated. During this distraction phase, the material that fills the gap is a soft, flexible tissue called "regenerate." It is made primarily of collagen, the main protein found in bone. This regenerate remains soft during this time because it lacks minerals. Hardening by mineralization occurs during the consolidation and healing phase.
Consolidation and healing phase
Once the lengthening process is complete, the bone enters the consolidation phase, where minerals are added to the regenerate, making it harder and more like normal bone. Over time, this new bone continues to remodel (a process where old or damaged bone is slowly broken down and removed, and new bone is built in its place) and becomes structurally the same as the original bone at both ends.

An adult patient, before and after limb lengthening surgery.
(Find a limb lengthening surgeon at HSS)
What types of limb lengthening procedures are there?
After the osteotomy that separates the bone into two halves, the gradual process of lengthening can be accomplished using either an internal lengthening nail or an external fixator.
The internal lengthening nail (ILN) is a telescopic, motorized intramedullary nail or rod that is inserted into the marrow cavity of the bone. By way of a remote control device controlled by the patient, the magnet in the nail is rotated. This gradually elongates the telescopic nail and the bone in which it is inserted. With this method, the bone is straightened at the time of surgery when the ILN is inserted, and the lengthening is then done gradually over the next several weeks.
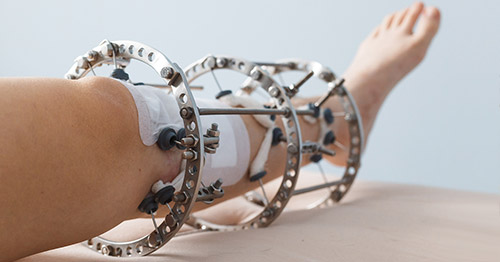
External fixation is a frame built on the outside of the limb connected to the bone via pins (rods), screws and wires. Adjustments to the external fixator can be used to gradually lengthen and straighten the short and malaligned limb. We use both monolateral (one-sided) and circular external fixation devices, depending on the patient.
 Pediatric patient before surgery, wearing the external fixator for leg lengthening, and after surgery.
Pediatric patient before surgery, wearing the external fixator for leg lengthening, and after surgery.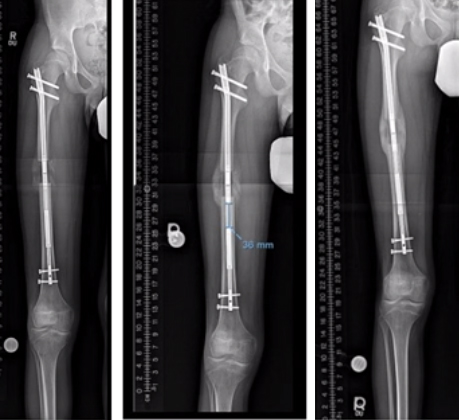 X-ray images of limb lengthening patient with internal nail lengthener at five weeks, where the bone has grown to desired length, at two months with bone growth consolidating, and at three months with completely healed bone.
X-ray images of limb lengthening patient with internal nail lengthener at five weeks, where the bone has grown to desired length, at two months with bone growth consolidating, and at three months with completely healed bone.What is the best method for limb lengthening?
Whenever possible, internal lengthening nail is the preferred device. However, there are many situations that require the use of the external fixator, including:
- in a growing child (whose growth plates remain open)
- for lengthening smaller bones of the foot, hand or arm
- for large limb deformities that cannot be straightened acutely using the internal nail
What is the recovery time for limb lengthening?
The exact duration depends on the amount of lengthening needed and varies among patients, but most people are walking without crutches after about two to three months. There are two phases of recovery:
- the distraction (lengthening) phase
- the consolidation and bone healing phase
Throughout recovery, physical therapy plays a crucial role in keeping the patient's joints flexible and in maintaining muscle strength. Patients are advised to eat a nutritious diet and to take calcium supplements. To hasten bone healing, gradual weight-bearing is encouraged, and the patient takes supplements like vitamin D3 and calcium to hasten bone healing.
During the lengthening phase, patients are mobile and walking with crutches. They also do daily exercises to maintain joint mobility and muscle strength. The recovery process gets much easier once the bone has grown to the full desired length. There is a gradual increase in weight bearing, and most people are walking without crutches after about two to three months.
The speed of bone healing is a function that differs by age, and the consolidation phase can last a considerable period – especially in adults. Children, generally, experience faster bone healing than do adults. As a general rule, children heal in half the time as it takes for adult patients.
For example, when the desired goal is 1½ inches of new bone growth, a child will wear the fixation device for three months. In adults, the use of the internal lengthening nail simplifies the process, since no external fixator must be worn, but the bone healing takes longer. Nevertheless, adult patients even in their 60s have had successful limb lengthening outcomes.
Who is eligible for limb lengthening surgery?
Treatment for limb length discrepancy should begin with a thorough evaluation from an orthopedic surgeon experienced in the procedure. Patients may be surprised to learn that what they thought was a discrepancy in leg length, for example, is actually an entirely different medical problem, such as scoliosis (an abnormal curve of the spine) or a hip deformity. Or, they may have a mistaken perception about the length of their limb length inequality. At Hospital for Special Surgery, orthopedic surgeons obtain a special series of X-rays to precisely assess and confirm each diagnosis.
When true discrepancy does exist, even when it is not the result of trauma, this asymmetry may lead to back, knee and ankle pain. In the case of malunion (a fracture that has not healed properly), osteoarthritis may develop. In some cases, a patient has lived with a limb length discrepancy for many years without experiencing problems and then develops troublesome symptoms in middle age.
In addition to meeting physical criteria for limb lengthening, it's important that the patient be highly motivated. Patients take an active role in their care, actually lengthening their bone with remote control adjustments, participating in physical therapy, and meeting with their physician in person or virtually every two to three weeks throughout the recovery process.
Limb lengthening surgery can be done safely and effectively in both children and adults–including those in their 20s, 30s, 40s, 50s, and even 60s. In pediatric patients, the orthopedic surgeon takes special care to avoid injuring the growth plate, and both normal growth and distraction osteogenesis continues during recovery.
In some cases, as with children who have congenital short femur, it may be advisable to address the problem in two stages. In this condition, the child has a percentage discrepancy that increases as they grow. For example, a two-inch discrepancy when the patient is first examined can be anticipated to increase to a three-inch discrepancy within five or six years.
Why you should choose HSS for femur lengthening
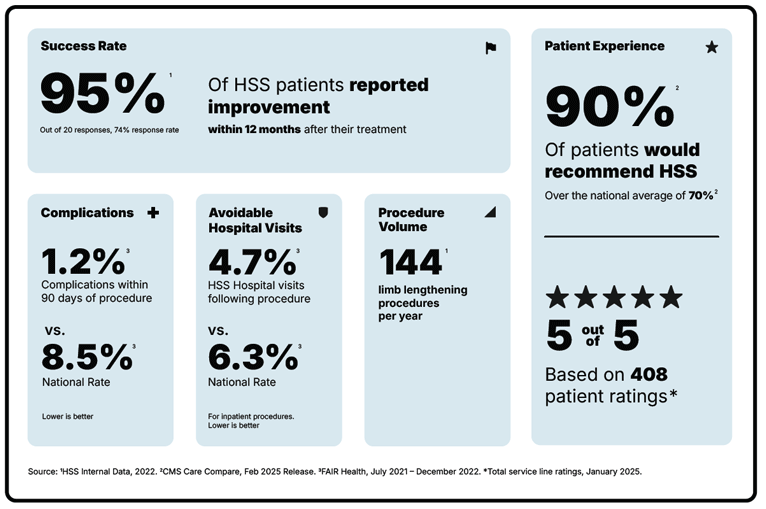
Limb lengthening of the femur is a surgery focused on improving your ability to walk and getting you back to the activities you love. But not all hospitals achieve the same results. Some are more reliable than others. With the help of the HSS Hospital Reliability Scorecard, you can make sure you're asking the critical questions to find the hospital that's right for you. Understanding the data points will help you make the best decision for your care. See hospital reliability data
Explore Related Patient Stories
View All Patient Stories
Emmanuel Tabi
Brooklyn, NY
Limb Lengthening Surgery
Don Davis
New Paltz, NY
Limb Lengthening Surgery

Laticia Nish
Jamaica, NY
Limb Lengthening Surgery
Eugene Devlin
Rye, NY
Limb Lengthening Surgery
Dov G.
Englewood, NJ
Limb Lengthening Surgery
Laura Carter
Gaithersburg, MD
Limb Lengthening Surgery
Michael Villane
Rumson, NJ
Limb Lengthening Surgery

Mim Baker Finkelstein
Stony Brook, NY
Limb Lengthening Surgery

Brett Harrison
Orange, CT
Limb Lengthening Surgery

Maddie McGovern
Nutley, NJ
Limb Lengthening Surgery

Michele McGuire
Perkasie, PA
Limb Lengthening Surgery
Vincent Annunziata
Sea Bright, NJ
Limb Lengthening Surgery

Rafael Aparicio
Darien, CT
Limb Lengthening Surgery

Daniel Bastian
Massapequa, NY
Limb Lengthening Surgery

Michael Gardner
Fort Worth, TX
Limb Lengthening Surgery

Avery Nobile
Southbury, CT
Limb Lengthening Surgery

Sidorela Lleshi
Queens, NY
Limb Lengthening Surgery

Kara Ryan
Chatham, NJ
Limb Lengthening Surgery

D. G.
Englewood, NJ
Limb Lengthening Surgery

Phillip
New York, NY
Limb Lengthening Surgery
References
- Fragomen AT, Fragomen FR. Distal femoral flexion deformity from growth disturbance treated with a two-level osteotomy and internal lengthening nail. Strategies Trauma Limb Reconstr. 2017 Nov;12(3):159-167. doi: 10.1007/s11751-017-0298-2. Epub 2017 Oct 16. PMID: 29039128; PMCID: PMC5653604. https://pubmed.ncbi.nlm.nih.gov/29039128/
- Galal S, Shin J, Principe P, Mehta R, Khabyeh-Hasbani N, Hamilton A, Fragomen A, Rozbruch SR. Humerus Lengthening: A Comparison of the Internal Lengthening Nail to External Fixation. HSS J. 2021 Jul;17(2):207-212. doi: 10.1177/1556331621996334. Epub 2021 Mar 4. PMID: 34421432; PMCID: PMC8361582. https://pubmed.ncbi.nlm.nih.gov/34421432/
- Goodbody C, Blyaker A, Widmann R, Dodwell E. Limb lengthening using the Ilizarov method or a monoplanar fixator. In: Flynn JM, Wiesel SW, editors. Operative techniques in pediatric orthopaedics. New York (NY): Wolters Kluwer; 2021. https://search.worldcat.org/title/654814414
- Goodbody CM, Buksbaum J, Harbison MD, Fragomen AT, Rozbruch SR. Limb Lengthening in Russell-Silver Syndrome: An Update Confirming Safe and Speedy Healing. J Pediatr Orthop. 2021 May 13. doi: 10.1097/BPO.0000000000001855. Epub ahead of print. PMID: 33999566. https://pubmed.ncbi.nlm.nih.gov/33999566/
- Hamdy RC, Bernstein M, Fragomen AT, Rozbruch SR. What's New in Limb Lengthening and Deformity Correction. J Bone Joint Surg Am. 2018 Aug 15;100(16):1436-1442. doi: 10.2106/JBJS.18.00584. PMID: 30106829. https://pubmed.ncbi.nlm.nih.gov/30106829/
- Rozbruch SR, Hamdy R, editors. Limb Lengthening and Reconstruction Surgery Case Atlas. Cham (CH): Springer International Publishing; 2020: doi:10.1007/978-3-319-02767-8.
- Rozbruch SR, Kleinman D, Fragomen AT, Ilizarov S. Limb lengthening and then insertion of an intramedullary nail: a case-matched comparison. Clin Orthop Relat Res. 2008 Dec;466(12):2923-32. doi: 10.1007/s11999-008-0509-8. Epub 2008 Sep 18. PMID: 18800209; PMCID: PMC2628243. https://pubmed.ncbi.nlm.nih.gov/18800209/
- Rozbruch SR, Pugsley JS, Fragomen AT, Ilizarov S. Repair of tibial nonunions and bone defects with the Taylor Spatial Frame. J Orthop Trauma. 2008 Feb;22(2):88-95. doi: 10.1097/BOT.0b013e318162ab49. PMID: 18349775. https://pubmed.ncbi.nlm.nih.gov/18349775/
- Rozbruch SR, Ilizarov S, Blyakher A. Knee arthrodesis with simultaneous lengthening using the Ilizarov method. J Orthop Trauma. 2005 Mar;19(3):171-9. doi: 10.1097/00005131-200503000-00004. PMID: 15758670. https://pubmed.ncbi.nlm.nih.gov/15758670/